


A Mixed Methods Study
Access resources tailored to your learning style
Getting Started with Dedoose
Review key features and terminology, data preparation tips, create a project and import data.
Learn More


Review key features and terminology, data preparation tips, create a project and import data.

A Mixed Methods Study
Our mixed methods study of an integrated breast and cervical cancer screening program in Cameroon, consists of several complex datasets, remote teams, multiple sites, multiple languages, and deeply detailed interviews. Although we have used other qualitative analysis tools in the past, and some of the team have used Dedoose individually, this was our first time using Dedoose as a team for a large-scale project. What stood out quickly was how much the platform supports real collaboration. Our team found the platform both user friendly and technically robust. The accessible help resources and online training sessions were also valuable, especially when learning to use advanced features. Our experience demonstrated how a well-designed analytic platform can enhance team-based qualitative inquiry and support the discovery of meaningful patterns within participant narratives.
Cervical and breast cancers remain the leading cancers among women in low- and middle- income countries (LMICs), with significant mortality due largely to late-stage diagnosis. In 2020, nearly 60% of new breast cancer cases and 73% of breast cancer deaths occurred in LMICs. In sub-Saharan Africa (SSA), the situation is particularly stark: up to 77% of breast cancer cases are diagnosed at advanced stages (1). For cervical cancer, while 60% LMICs have official cervical screening recommendations, only 33% of African countries have implemented these guidelines (2) and cervical cancer screening coverage remains extremely low ranging from 0.4% to 25%, with a pooled uptake of just 12.87% (3-5).
In this study, we are working with the largest health system in Cameroon that runs the country’s most comprehensive women’s cancer prevention programs. It offers a four-prong approach; 1. Cervical cancer screening; 2. Breast cancer screening; 3. Family planning; and 4. Syndromic STI management. The focus of our project is specifically on breast and cervical cancer components because they uniquely integrate these services.
The study aims to evaluate this integrated breast and cervical cancer screening program via the implementation of the science RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance) framework. Qualitative interviews were conducted with patients and nurses and clinic coordinators to better understand the program’s implementation and maintenance components.
Ethical approval for this study was obtained through multiple institution IRBs. Participant recruitment and informed consent were conducted voluntarily. Between March and September 2024, a research team unaffiliated with the clinics conducted in-depth, semi-structured interviews with 25 patients, 30 nurses and 13 coordinators. The sample size study was based on the thematic saturation of the data. Patient interviews were carried out immediately after they completed screening appointments. The interviews were:
• Conducted in French, English, or Pidgin
• Led by a multilingual Cameroonian medical anthropologist
• Held in private spaces within clinics
• Audio-recorded, transcribed, and translated when necessary
The tailored interview guides explored patient-centered aspects of receiving integrated screening, including expectations, communication, comfort, and perceptions of the service. Nurses were asked for their perspective on, among other things, any challenges with the program, perceived barriers and facilitators to screening, their work environment, work relationships, training and support, and recommendations. The clinic coordinator interviews focused on how coordinators attained their role, challenges with integrated screening, training and support, infrastructure, team dynamics, and recommendations.
All responses were recorded verbatim. The data were deidentified to protect participant anonymity and confidentiality. Once transcribed and translated, thematerials were prepared for qualitative coding. That’s when we opened Dedoose.
All the transcripts were uploaded to Dedoose, and a codebook was developed from a randomly selected subset of the transcripts and the interview guide for each group of interviewees (patient, nurse, coordinator). Dedoose’s ability to bulk upload a full codebook made the initial setup fast and smooth, something our team particularly appreciated.
Coding was done both deductively, informed by the study’s research questions, and inductively, allowing for any novel insights to emerge from the data. Each interview transcript was coded line-by-line and iteratively reviewed using the developed codebook by two independent coders. The two coders met regularly during the coding process to maintain continuity and consensus, to enhance analytic rigor and coherence. This process facilitated the identification and organization of overarching themes that captured salient patterns across participants’ accounts. If there were coding discrepancies, a third independent coder reviewed the transcript.
Although we had worked with other qualitative platforms before and some of us were familiar with Dedoose on an individual basis, this was our first time using Dedoose as a team for a multi-coder project. It quickly became clear that the platform was built with team-based research in mind.

The platform’s design supported a collaborative workflow without sacrificing analytic rigor. One of the features we valued and relied on the most was the ability for coders to work independently without seeing each other’s coding during the first pass. This feature makes Dedoose stand out from other mixed method analysis platforms, and allowed for:
• Unbiased individual coding
• Clear, structured code comparison
• Efficient resolution of discrepancies
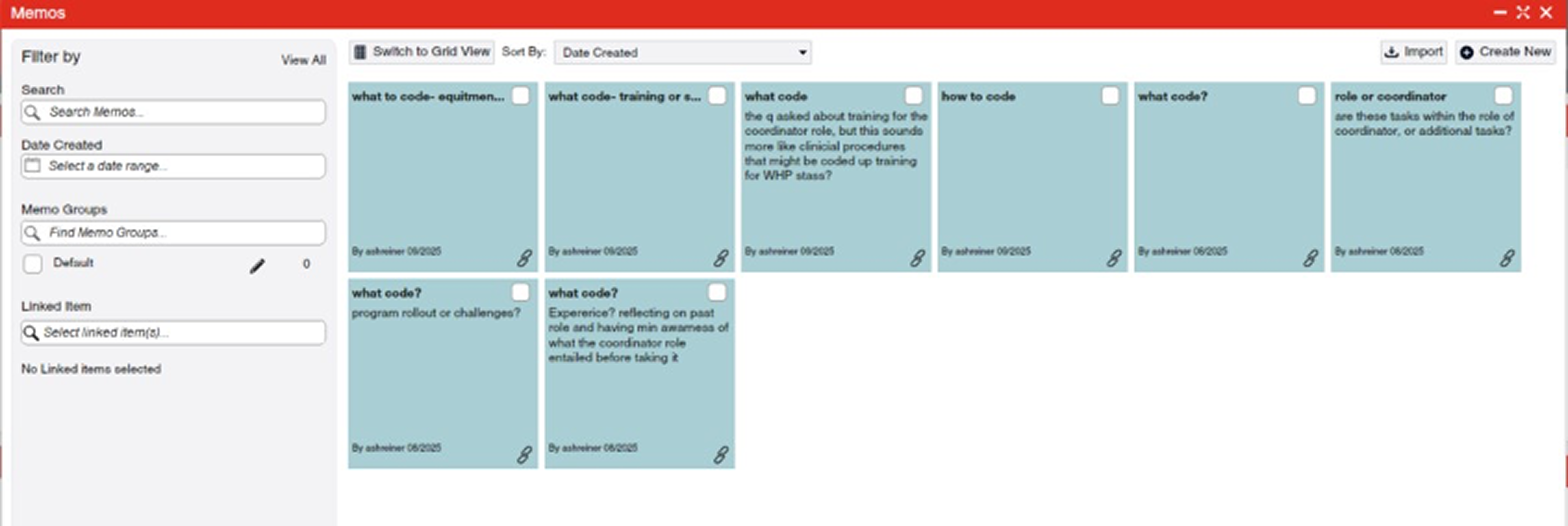
• Transparent decision-making through memos and notes
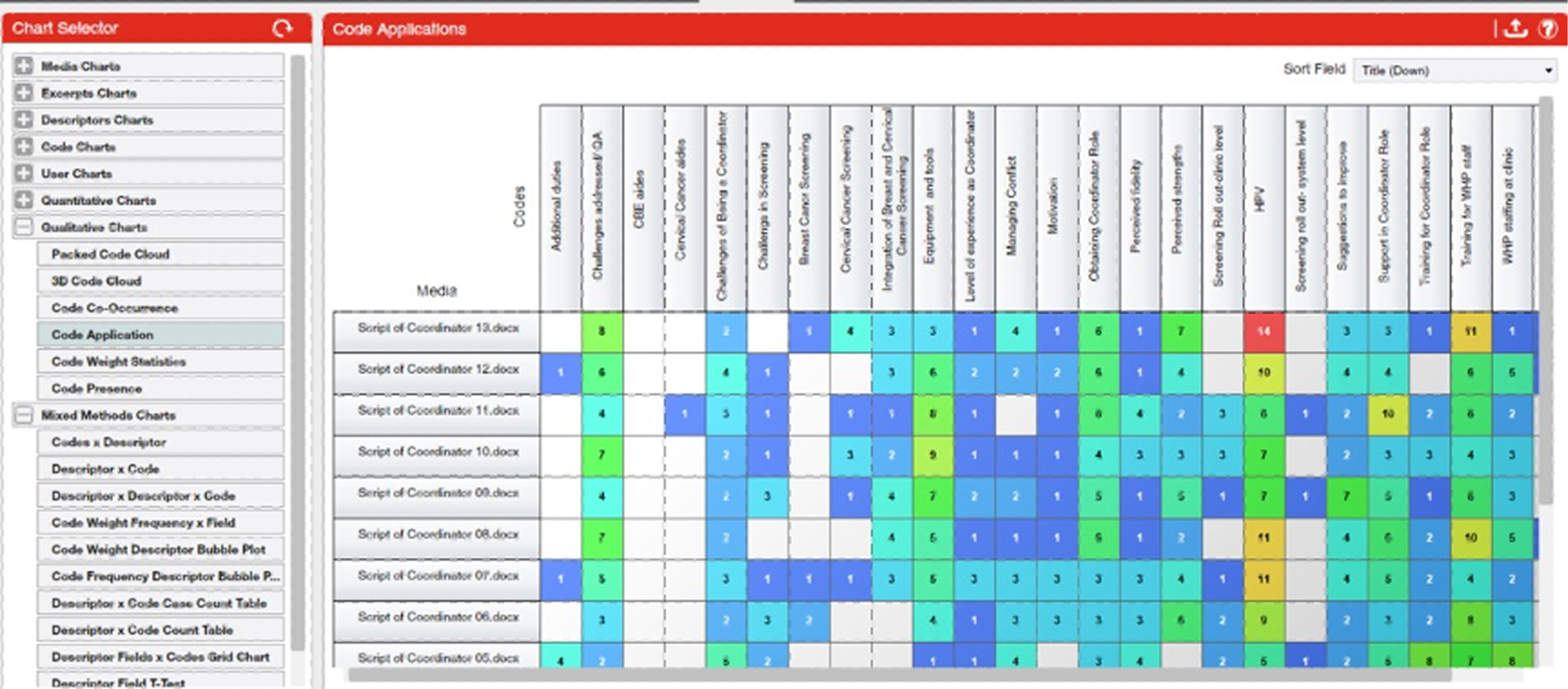
We also explored Dedoose’s visualization tools, which helped us keep track of coding progress and understand how codes were distributed across transcripts and sites. The organizational value of those visual tools played helped shape how we reviewed the data and prepared for later analytical stages.

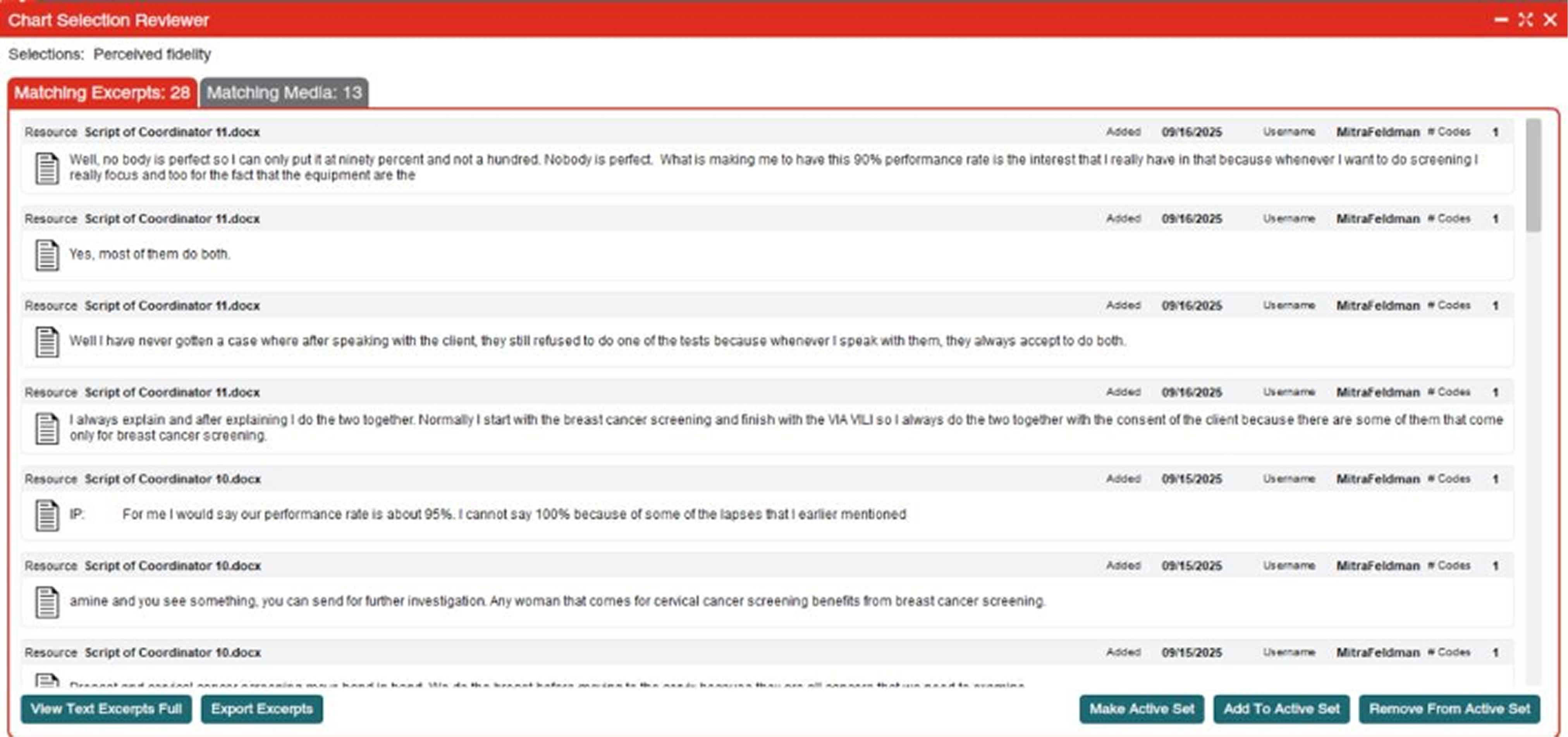
Exporting coded excerpts, code applications, and analytic tables into formats like Excel and Word made it easy to transition from coding to interpretation and writing. Having these materials neatly organized saved our team hours of manual formatting and administrative work.
Several aspects of Dedoose stood out as especially helpful for this project:
• Multi-coder functionality that supports independent work without confusion
• Clear code comparison dashboards
• Memos and notes that stay anchored to excerpts
• Bulk codebook uploads that speed up setup
• Intuitive visuals for monitoring progress
• Responsive user support and online training
• Exporting to Excel or Word
We found the platform both user-friendly and powerful; easy enough to learn quickly, but robust enough for a multi-site, multilingual research project.
Based on our experience, we’d offer a few suggestions:
• Spend time exploring the platform early in the project. Many helpful tools aren’t immediately obvious.
• Take advantage of Dedoose’s online training sessions and tutorials. They’re short, practical, and genuinely helpful.
• Be intentional when creating your codebook. A well-thought-out code structure makes collaborative coding far smoother.
• Use memos frequently. They keep analytic thinking organized and make team discussions more grounded.
Our study focused on understanding the patients’, providers’ and administrators’ experiences with integrated breast and cervical cancer screening in a resource-limited environment. While the content of the interviews was rich and meaningful, the process of analyzing them required a platform that could handle complexity, collaboration, and structure. Dedoose played a central role in helping our research team analyze this dataset with rigor, clarity, and collaboration. Its features supported efficient coding, facilitated team communication, and enabled clear identification of patterns across diverse patient narratives. For researchers working with complex qualitative data, and especially those conducting team-based analysis, Dedoose offers a powerful and intuitive platform for generating meaningful insights that can be used to help inform public health practice.
1. Ebrahimoghli R, Aghaei MH, Azami-Aghdash S, Houssami N. Uptake of breast cancer screening practices in low- and middle-income countries: a systematic review andmeta-analysis. J Natl Cancer Inst. 2025;117(1):29-39.
2. Bruni L, Serrano B, Roura E, Alemany L, Cowan M, Herrero R, et al. Cervical cancer screening programmes and age-specific coverage estimates for 202 countries and territories worldwide: a review and synthetic analysis. The Lancet GlobalHealth.
2022;10(8):e1115-e27.
3. Gakidou E, Nordhagen S, Obermeyer Z. Coverage of cervical cancer screening in 57countries: low average levels and large inequalities. PLoS Med. 2008;5(6):e132.
4. Hausiku L, Kouame K, Aboua YG. Perceptions and attitude of women of Luderitz, Namibiaon Pap smear and cervical cancer prevention. BMC Womens Health. 2022;22(1):126.
5. Yimer NB, Mohammed MA, Solomon K, Tadese M, Grutzmacher S, Meikena HK, et al.Cervical cancer screening uptake in Sub-Saharan Africa: a systematic review and meta-analysis. Public Health. 2021;195:105-11.
Dr. Lily Gutnik joined the UAB Division of Breast and Endocrine Surgery in November 2021 as an assistant professor. She also supports the General Surgery Residency Program as assistant program director for global surgery. Additionally, Dr. Gutnik serves the O'Neal Comprehensive Cancer Center at UAB as an associate scientist in the Cancer Control and Population Science Program. In 2022, she was appointed to the Sparkman Center for Global Health Scholars Program. She is the inaugural Associate Vice Chair of Global Surgery, helping build and expand UAB's global collaborations.
Dr. Gutnik completed her undergraduate degree at New York University and her Medical Degree at the Medical School for International Health—a collaboration between Ben Gurion University in Israel and Columbia University in New York. She also holds a Masters in Public Health from Harvard University.
Dr. Gutnik completed a research fellowship at the Center for Surgery and Public Health at Harvard University/Brigham and Women's Hospital where she gained valuable experience in health services research. Dr. Gutnik served on the Finance and Economics Committee of the Lancet Commission for Global Surgery. Her longstanding research passion has revolved around the impact of breast cancer screening and early detection in low-resource settings, particularly in Sub-Saharan Africa. Her research is supported by ASCO, NIH, and industry partners.
Dr. Gutnik was previously a Fulbright and Fogarty Fellow in Lilongwe, Malawi where she established and evaluated the efficacy of Malawi’s first breast cancer screening initiative by activating laywomen to become trained breast health workers. In addition, she serves in an advisory board member for international NGOs: (i) Know Your Lemons, which focuses on education and awareness materials; (ii) Kibir Desta- providing quality cancer care to underserved populations in Ethiopia. She is a committee member of PreTac—a franchisee of Discovering Hands in Geneva, Switzerland which focuses on training blind women to become clinical breast examiners. She was a UICC Young Leader in 2023-24 cohort and Birminham Business Journal 40 under 40 honoree.