From Hospital Lessons to Home Recovery: What Caregiver Conversations Taught Us (and How Dedoose Helped Us See the Patterns)
Dr. Poornima Sharma
Dedoose Series
5 min
From Hospital Lessons to Home Recovery: What Caregiver Conversations Taught Us (and How Dedoose Helped Us See the Patterns)
From Hospital Lessons to Home Recovery: What Caregiver Conversations Taught Us
Introduction
When someone undergoes cardiac surgery, the most critical part of recovery often begins after they leave the hospital.
In many of the contexts where we work at Noora Health, families—not just patients—carry the responsibility of recovery. A spouse reminds them to take medicines. A daughter monitors wound care. A sibling helps them go to a follow-up visit.
Our intervention, the Care Companion Program (CCP), is a caregiver education program that trains family members on critical care skills through structured group sessions, demonstrations, and practical guidance delivered in hospitals, local clinics, and community settings. The cardiac program focuses on essential recovery behaviors—such as medication adherence, hygiene, nutrition, and danger sign recognition—so that caregivers feel more confident supporting patients at home.
We wanted to better understand participants’ experiences with CCP beyond the hospital setting—how prepared patients and caregivers felt after the sessions, what recovery actually looked like at home, and if and how CCP influenced everyday care practices.
To explore this, we conducted an explanatory sequential mixed-methods design, combining a quasi-experimental pre–post quantitative evaluation with qualitative inquiry, with cardiac patients and their caregivers in a tertiary care hospital in South India. What followed was not just a research exercise—it became a learning journey about how people interpret guidance, how caregivers build confidence, and how qualitative tools can help transform conversations into insight.
Starting with Conversations, Not Metrics
Many health programs are evaluated using numbers: readmission rates, follow-up visits, or adherence scores. While these indicators are essential, they don’t always explain why behaviors change—or why they don’t.
For this study, we wanted to step into the lived experiences of patients and caregivers.
We designed a set of in-depth interviews to understand:
How patients and caregivers experienced CCP sessions during hospitalization
Whether they felt prepared for discharge
What recovery looked like once they returned home
How caregivers supported daily post-operative care
What challenges did families face after returning home
Instead of structured surveys, we chose semi-structured interviews. This allowed conversations to flow naturally while still covering key themes.
In total, we interviewed 13 cardiac patients and 12 caregivers, speaking to them separately so each could share their perspective openly.
Most interviews were conducted in Kannada and later translated into English. All of them took place in participants’ homes, which helped us observe the real environments where recovery was happening—but also introduced unpredictability.
Phones rang. Family members walked in and out. Patients sometimes became tired mid-conversation.
And that, in many ways, was exactly the point.
Recovery does not happen in controlled environments—and neither should research about it.
The Challenge of Capturing Real Experiences
One of the most interesting aspects of the study was also one of the most difficult.
Not every participant found it easy to describe their experiences in detail.
Some responses were brief:
“Yes, we followed it.” “Yes, the session was helpful.” “Yes, we give medicines on time.”
While these responses were positive, they required deeper probing to understand what “helpful” actually meant in practice.
Other challenges also emerged:
Some participants struggled to recall details of CCP sessions after discharge
Patients were still physically recovering during interviews
Scheduling home visits required flexibility and multiple follow-ups
Despite these constraints, clear patterns began to emerge about how recovery unfolded at home.
Caregivers played a central role in recovery, reinforcing CCP learnings through daily support and helping patients follow recommended post-operative behaviors at home.
Adherence was generally strong, driven by caregiver involvement and patient motivation, though financial and access barriers continued to affect consistent follow-up care for some families.
These stories highlighted something important: education does not translate into behavior automatically—it translates through context.
To make sense of these patterns across interviews, we needed a structured way to analyze the data.
When the Transcripts Start to Pile Up
After transcription and translation, we had dozens of pages of qualitative data.
Reading individual interviews was insightful—but patterns across interviews were harder to track.
We developed a collaborative codebook based on both our research questions and early transcript review.
Themes included:
Discharge preparedness
Caregiver confidence
Behavior adoption
Barriers to care
Health system interactions
At this stage, we moved our workflow into Dedoose.
How Dedoose Helped Us See What We Might Have Missed
Qualitative analysis often involves moving between detailed reading and pattern recognition. One of the biggest advantages of Dedoose was how it helped us do both efficiently.
Bringing Everything into One Place
Uploading all transcripts into a single platform immediately made the dataset easier to navigate. Instead of working across multiple documents, the team could access interviews centrally and apply codes consistently.
This was especially useful given the translated nature of the dataset—we frequently revisited excerpts to ensure interpretation accuracy.
Making Coding Iterative (Without Losing Structure)
Like most qualitative projects, our coding evolved over time.
Some codes were merged. Others were refined. Definitions became sharper as patterns emerged.
Dedoose allowed us to update the codebook without disrupting earlier work, making iteration much smoother than document-based workflows.
Discovering Patterns Through Visualization
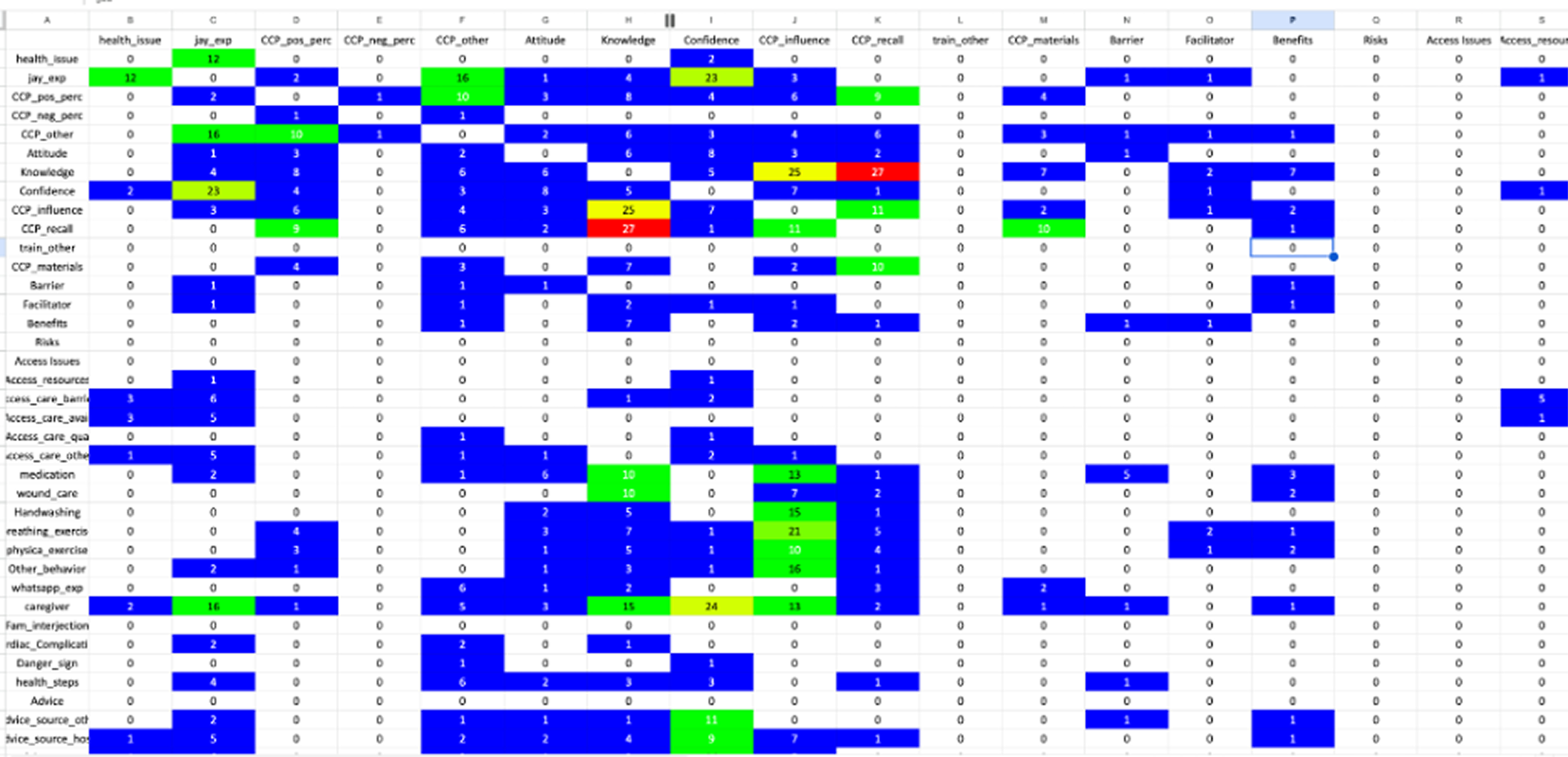
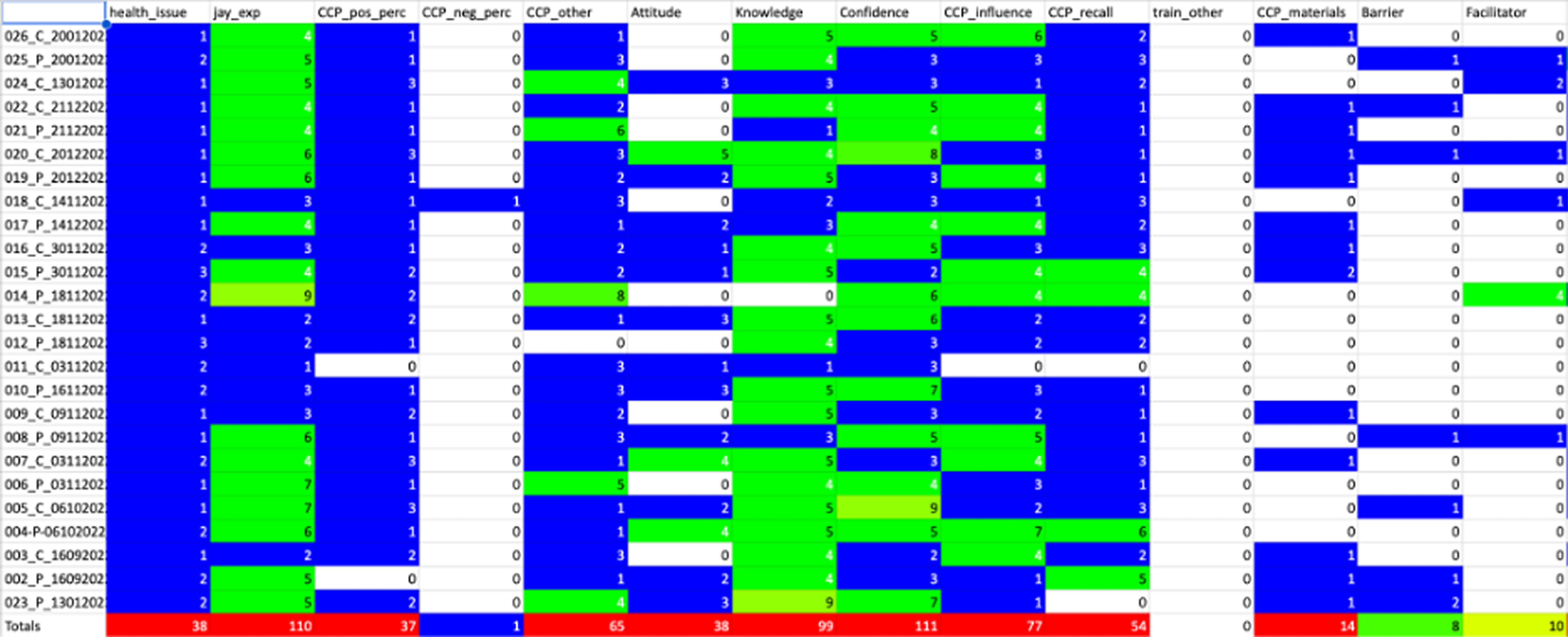
One feature that became particularly valuable was code co-occurrence visualization.
Rather than manually scanning transcripts to identify relationships, we could quickly see which themes appeared together most frequently.
For example:
CCP often appeared with knowledge
Caregivers appeared alongside behavior adoption like wound care
These visual patterns helped us move from descriptive summaries toward deeper interpretation.
It also helped guide internal research discussions—turning “interesting observations” into structured insights.
Making Synthesis Easier (and Faster)
Another practical benefit was the ability to export coded excerpts by theme.
This became extremely useful when drafting synthesis notes and comparing responses across patients and caregivers.
Instead of searching across transcripts repeatedly, we could review all excerpts under a theme in one place.
For qualitative teams working under time constraints, this workflow improvement alone made a significant difference.
Lessons We Learned Along the Way
Every research project teaches methodological lessons—and this one was no exception.
Visualize Earlier Than You Think
Initially, we began using visualization tools later in the coding process. Once we started using them earlier, patterns surfaced faster and helped refine our coding strategy.
Early visualization saved time downstream.
Codebook Alignment Is Worth the Time
Investing time upfront to collaboratively define codes improved consistency across researchers.
Even small clarifications—like distinguishing between confidence and understanding—reduced ambiguity during coding.
Translation Adds Analytical Depth
Because transcripts were translated from Kannada to English, interpretation required additional context discussions.
Interestingly, this process strengthened the analysis by encouraging closer reading and team reflection.
Advice for New Dedoose Users
For researchers beginning their qualitative analysis journey—or transitioning from document-based workflows—here are a few practical suggestions:
Start small. Code a few transcripts first and refine your codebook before scaling.
Use visualization tools early. They help surface relationships that are difficult to detect through reading alone.
Document decisions as you go. Analytic clarity improves when interpretation steps are recorded.
Treat qualitative software as a thinking partner. The goal is not just organization—it is insight.
Why This Work Matters
One of the most powerful takeaways from this study was a reminder that recovery is rarely an individual process—it is a family process.
Caregivers interpret instructions, adapt them to real-life constraints, and sustain behaviors long after discharge.
Understanding that process requires listening carefully—and analyzing thoughtfully.
Tools like Dedoose help structure that listening.
And when qualitative insights are translated into program improvements, they help ensure that hospital education does not stop at the hospital—it continues into the everyday routines that shape recovery.
Author Bio
Poornima Sharma is a Cross-Country Research Manager at Noora Health, where she leads multi-country research and evaluation of digital and hospital-based interventions that support patients and caregivers in low-resource settings. Her work sits at the intersection of behaviour change science, mixed-methods research, gender-sensitive evaluation, digital health, and AI evaluation in healthcare, with a strong focus on translating evidence into practical program improvements. A trained Dental Surgeon with a Master’s in Public Health, she specializes in evidence generation, implementation science, and human-centered evaluation, with particular interest in how gender and caregiving dynamics shape health behaviours and outcomes.
Poornima is known for her empathetic leadership and systems-focused approach to research, combining behavioural insights, stakeholder engagement, and data-driven decision-making across global health programs in Southeast Asia and Australia. Grounded in lived experiences of caregiving and mental health, her work emphasizes equity, compassion, and real-world impact. She is currently focused on evaluating AI systems in healthcare and building practical evaluation frameworks that help translate research into stronger, more inclusive health systems.